
Utilizing Artificial Intelligence
To Automate Prediction of the Radiographic Sharp Score in Reumatoid Arthritis
Score Prediction
The machine learning model that we built calculates the Sharp Score from images without the need for a radiologist and converts it to a clinical DAS28, which is used by physicians to monitor disease activity.

Novelty:
Automation of Sharp Score for Rheumatoid Arthritis (RA) and Conversion from Radiographic Sharp Score to Clinical DAS28.
Utilization: Assist clinicians, primarily radiologists, rheumatologists and physicians, to confirm diagnosis and treatment of rheumatic disease.
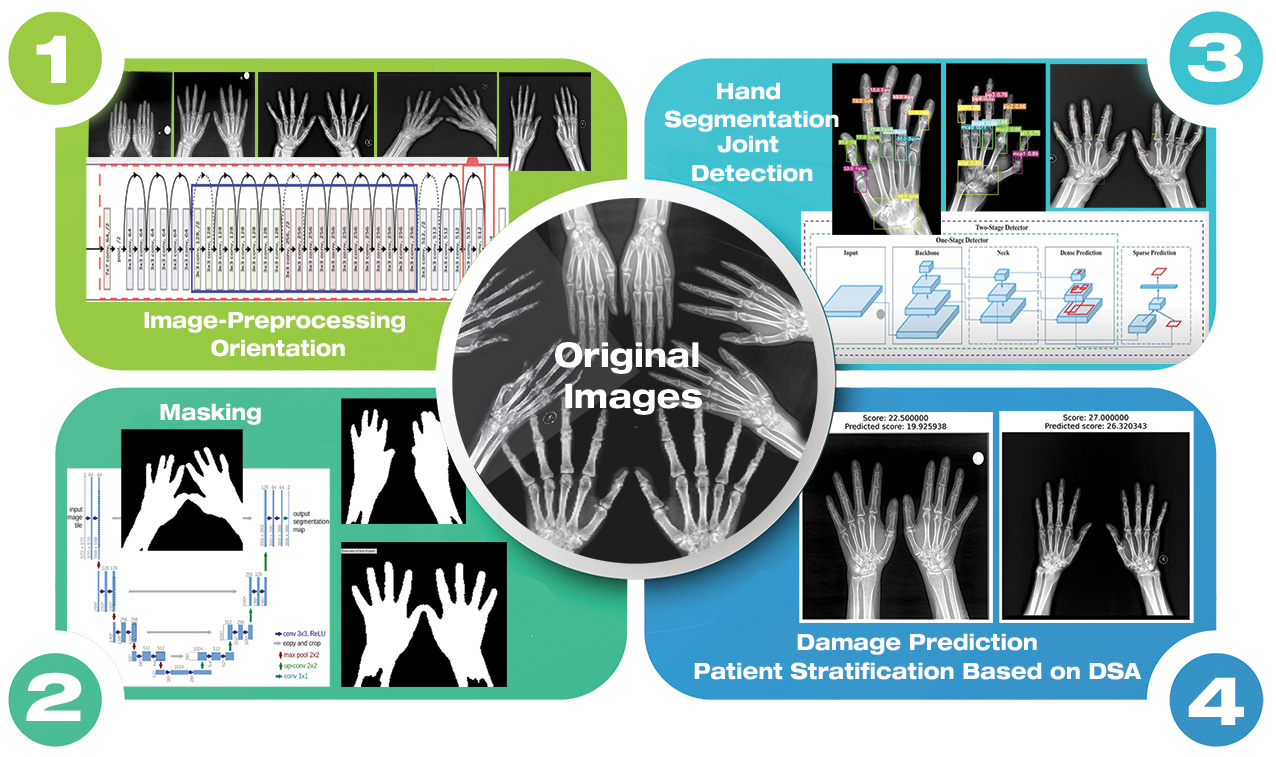
Image Manipulation
Image-preprocessing orientation, masking, hand segmentation, join detection, damage prediction, patient stratification based on DSA.
Compelling, Urgent Need for Automated Scoring of RA in Radiographic Joint Damage
Joint damage found in radiographic images is an important measure of clinical outcome in RA, which is difficult to study because of feasibility issues. Currently, despite the large amount of radiographic data available at hospitals, such a tool doesn’t exist because the scoring is labor-intensive and requires highly skilled personnel.
Current state-of-the art scoring involves visual inspection and equires extensive expertise/training and two readers to assess inter-observer variability.
Impact Clinical usage: At Ayass Research Institute, LLC, we believe a model based radiographic image analyzer will be an essential tool for RA scoring on a large-scale of thousands to millions, which is difficult to achieve with human scoring. Integrating genomic and radiomics models will build a powerful tool for precision medicine.
Significance of Our Work for RA
Structural damage, assessed on plain films, can indeed be used as a surrogate for clinical outcome.
RA affects 0.5–1% of the global population and is associated with disability, work loss, and premature death. In the USA, this equates to a cost of $19.3 billion annually in both healthcare and indirect expenses.
There is more and more evidence available from clinical trials and cohort studies of a clear relation between inflammation (disease activity) and structural damage, as well as a relation between structural damage and clinical outcome.
There is a relation between the response to treatment when measured as clinical disease activity and when measured as radiographic progression in most clinical therapeutic trials. This is robust evidence for the hypothesis that inflammation leads to structural damage.

Joint damage scoring Sharp/van der Heijde
The Sharp/van der Heijde (SvdH) method quantifies erosion and joint space narrowing (JSN). The method assesses the joints in both hands (all MCPs, 1st IP, all PIPs, scaphoradial, lunate, radial, distal ulna, and trapeziometacarpal) and feet (all MTPJs and 1st IPJ).
Sixteen areas from each hand and six areas in each foot are included in the erosion score, ranging from 0 to 5. JSN is assessed at 15 areas from each hand and six areas from each foot, ranging from 0 to 4. Since we only used the SvdH method to assess the hands; overall scores thus ranged from 0 to 280.
The SvdH method for RA scoring has been used to evaluate treatment in several studies of biologic agents and has shown good sensitivity and reliability.

Sharp/van der Heijde (SvdH) Scoring Method
The erosion score per joint of the hands can range from 0 to 5.
Erosions are scored 1 if they are discrete but clearly present, and 2 or 3 if they are larger, depending on the surface area of the joint involved.
A score of 4 is given if the erosion is large and extends over the imaginary middle of the bone.
A score of 5 is given if a complete collapse of the joint is present or if the full surface of the joint is affected.
The maximal erosion score for each hand is thus 80, considering the 16 areas for erosions per hand.
EROSIONS: 1 = Discrete lesion, 2-4 = Surface dependant, 3 = Reaches >50% of the joint surface, 5 = Bone collapsus

Sharp/van der Heijde (SvH) Scoring Method
Joint space narrowing and joint subluxation or luxation are combined in a single score with a range of 0 to 4. A normal joint space is scored 0.
A score of 1 is allowed when there is focal narrowing of the joint or when the joint space is not sufficiently narrowed to be scored 2.
The score of 1 should not be used when the reader is unsure whether there is joint space narrowing. A generalized narrowing leaving more than 50% of the original joint space present is scored 2. A generalized narrowing leaving less than 50% of the original joint space present is scored 3, and a subluxation of a joint is also scored 3. A bony ankylosis or a complete luxation of the joint is scored 4. The maximal narrowing/(sub)luxation score for each hand is thus 60.
JOINT SPACE NARROWING: 1 = Focal or not important enough to quote 2, 2 = >50% space left (generalized narrowing), 3 = <50% space left or subluxation, 4 = Complete ankylosis or luxation.